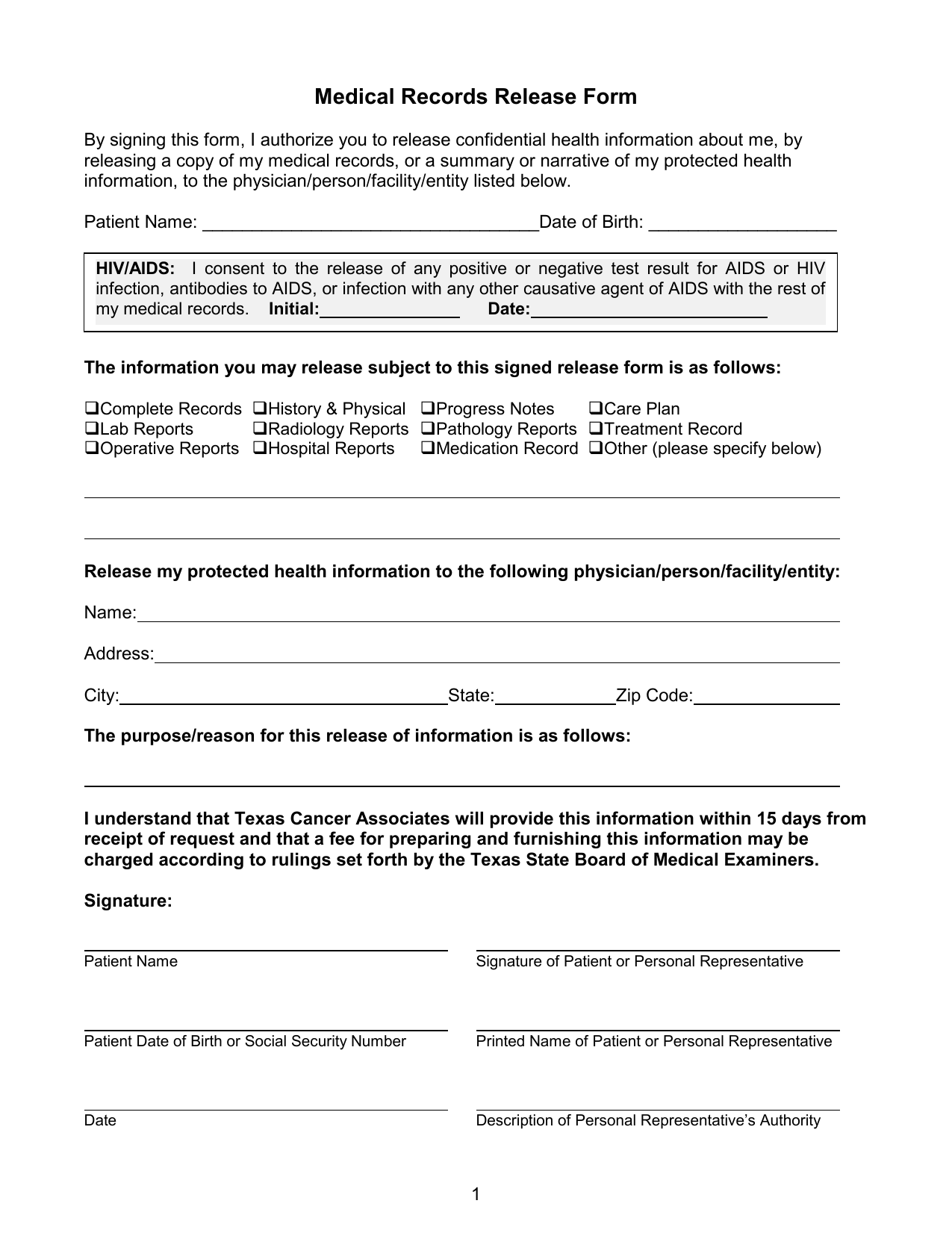
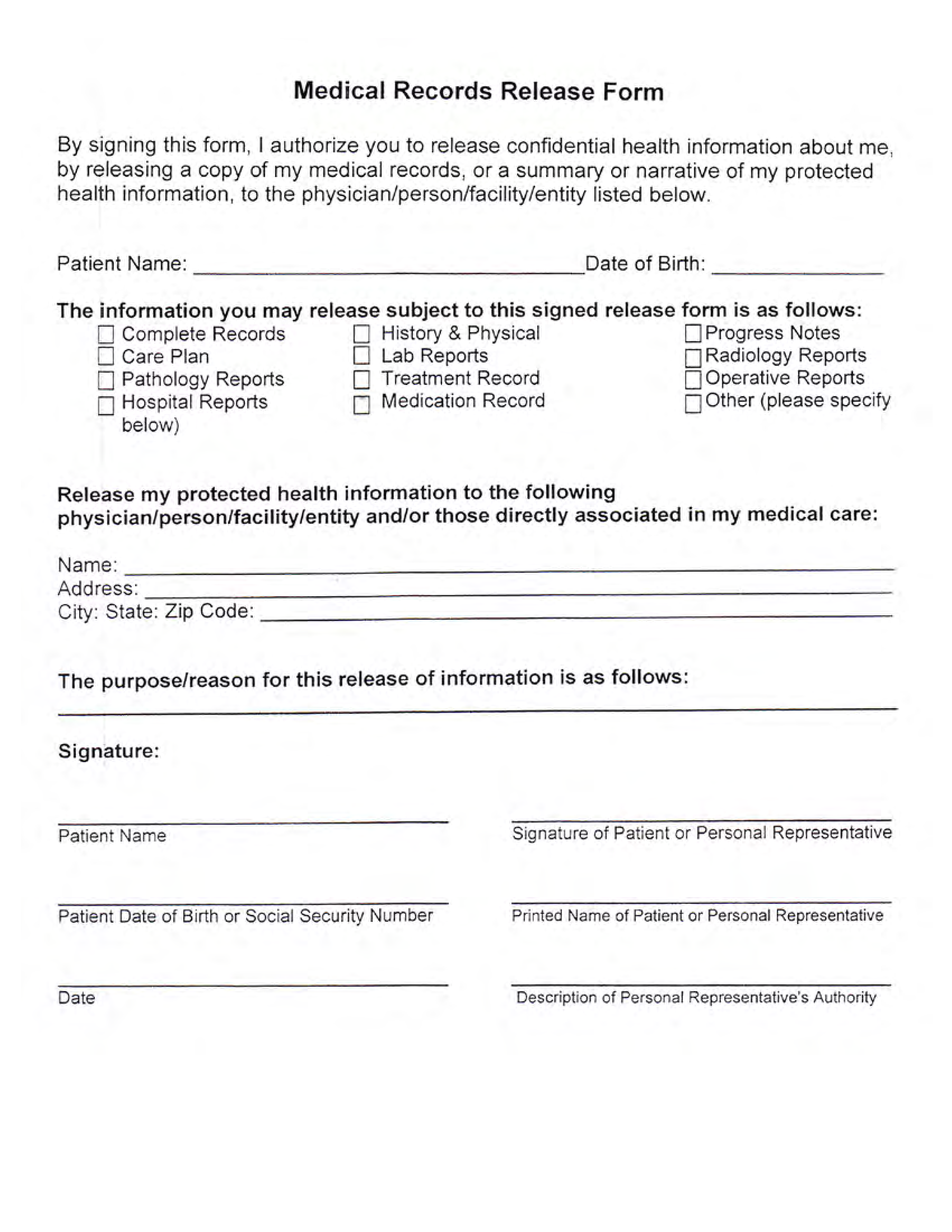
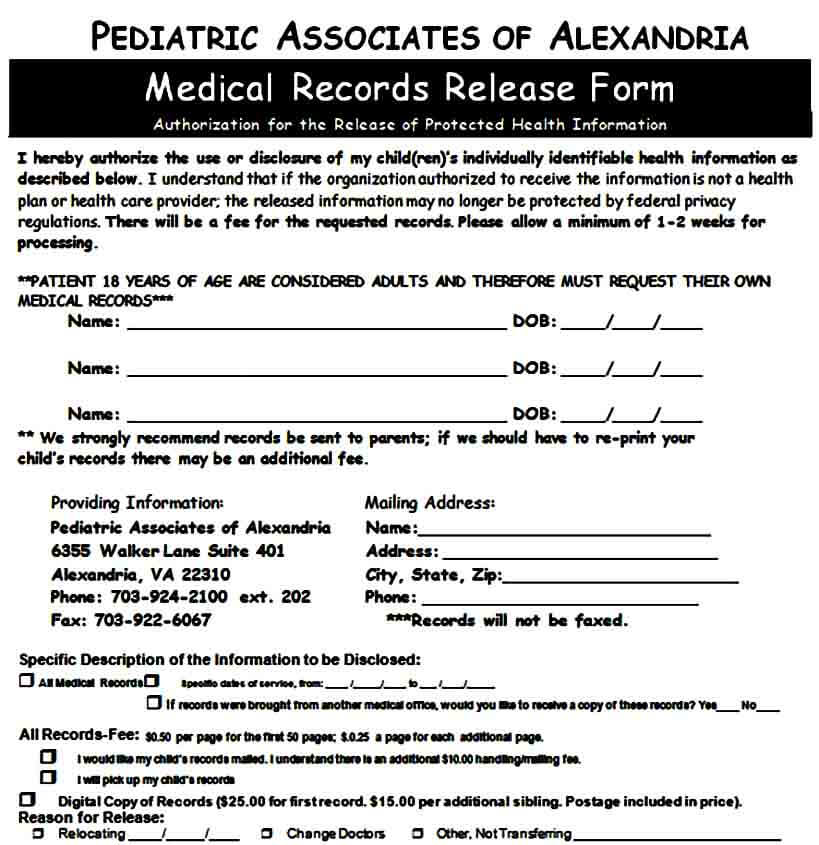
Medical Records Release Form Printable - This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. A patient can also request their medical records not currently in their possession. It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. I authorize ________________________ (“authorized party”). The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. It also allows the added option for healthcare providers to share information.
The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. It also allows the added option for healthcare providers to share information. A patient can also request their medical records not currently in their possession. I authorize ________________________ (“authorized party”). This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards.
This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. I authorize ________________________ (“authorized party”). It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. A patient can also request their medical records not currently in their possession. It also allows the added option for healthcare providers to share information. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party.
Medical Records Release Form templates free printable
The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. I authorize ________________________ (“authorized party”). It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. Write a medical records release authorization letter to the relevant office requesting the release, access,.

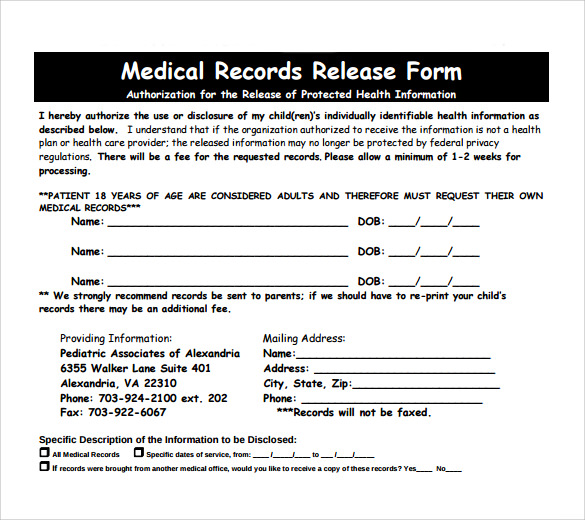
Pdf Printable Blank Medical Records Release Form
Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. This form is for use when such authorization is required and complies with the health insurance portability and.
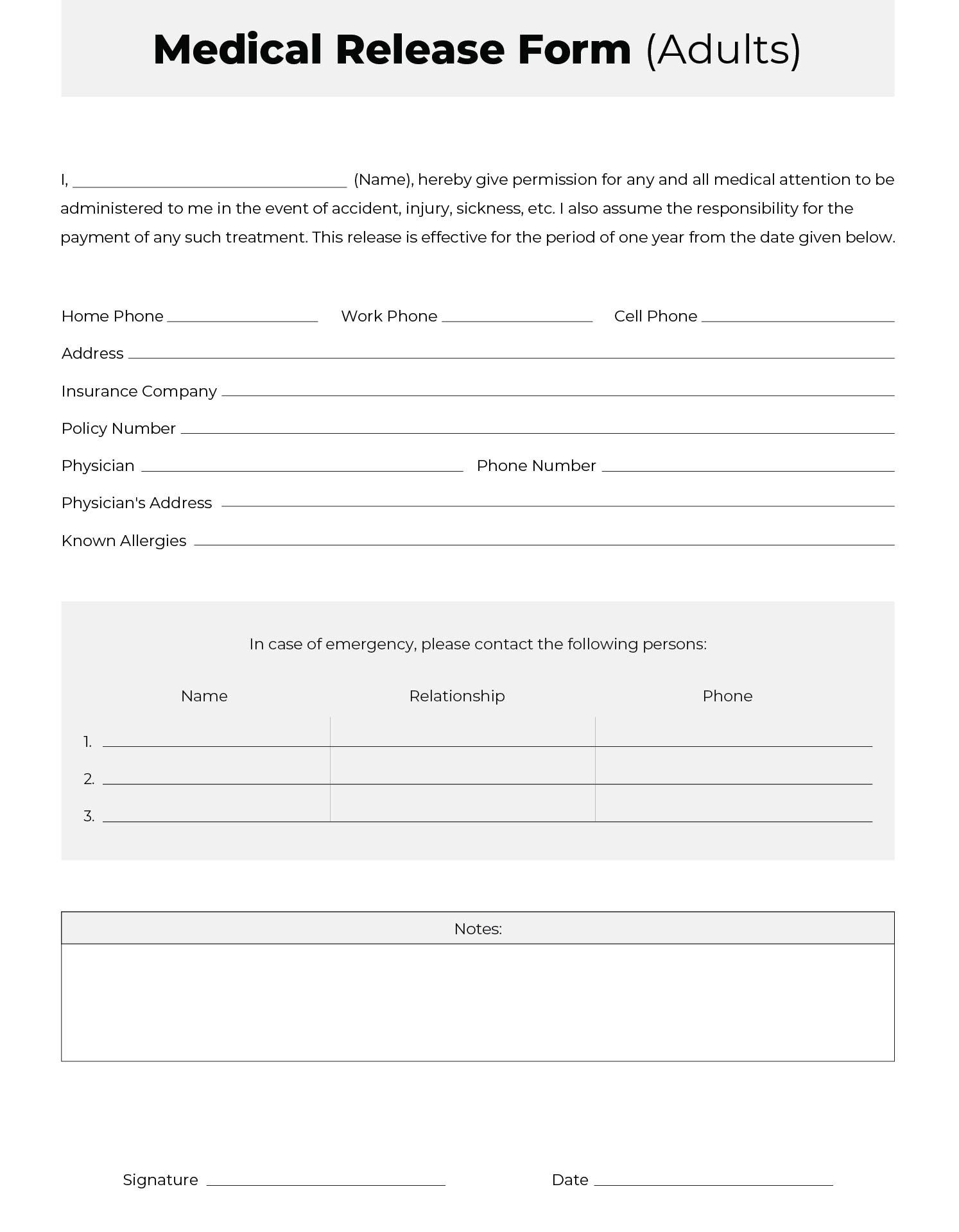
Medical Release Form Printable Adult
It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. The medical record information release (hipaa) form allows patients to give authorization to a 3rd party.
Printable Medical Records Release Form Templates at
It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. I authorize ________________________ (“authorized party”). A patient can also request their medical records not currently in.
Medical Records Release Form Printable
I authorize ________________________ (“authorized party”). The medical record information release (hipaa) form allows patients to give authorization to a 3rd party and access their health records. It also allows the added option for healthcare providers to share information. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. A medical.
Sample Medical Records Release Form Mous Syusa
A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. It is essential to follow the state’s guidelines on how to craft the.
FREE 10+ Medical Records Release Forms in PDF
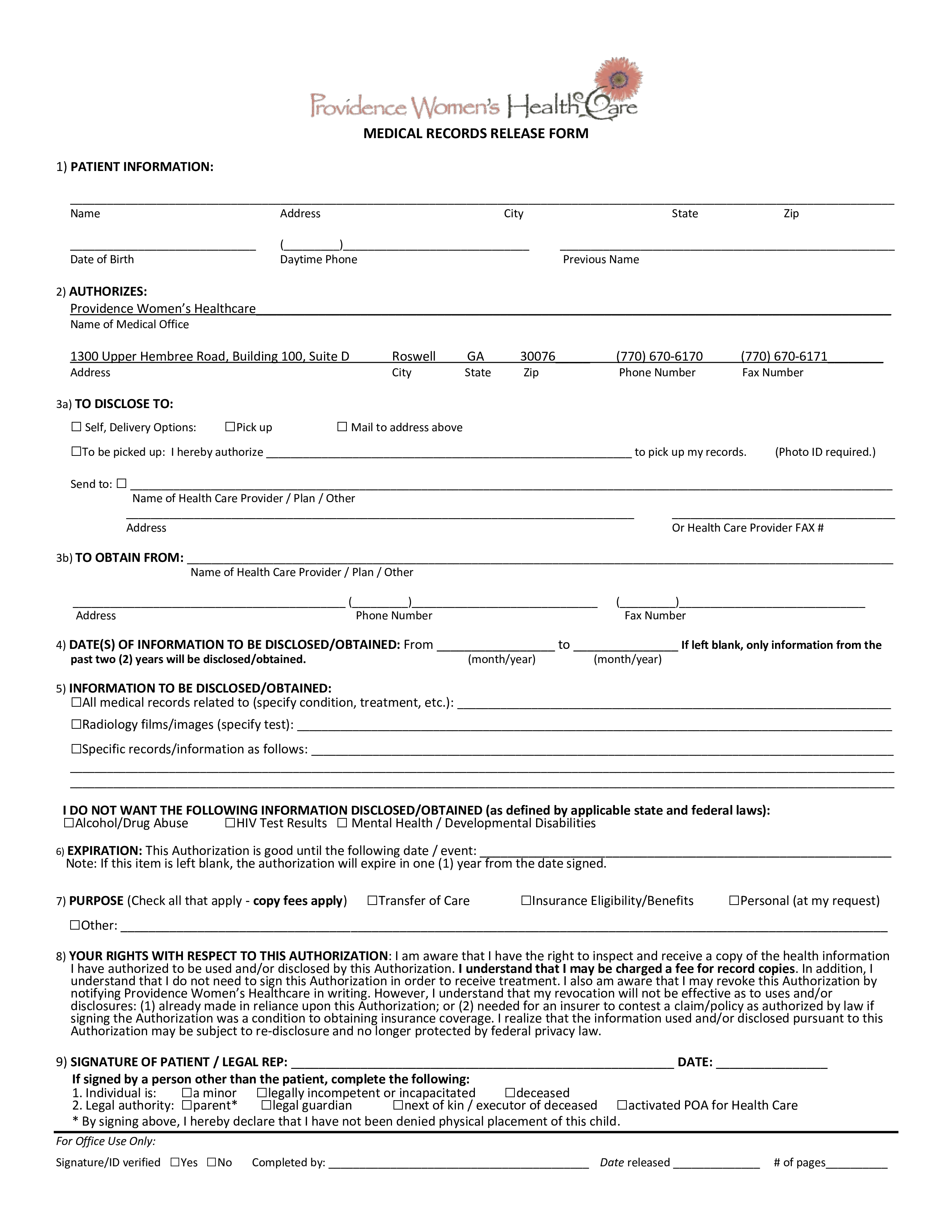
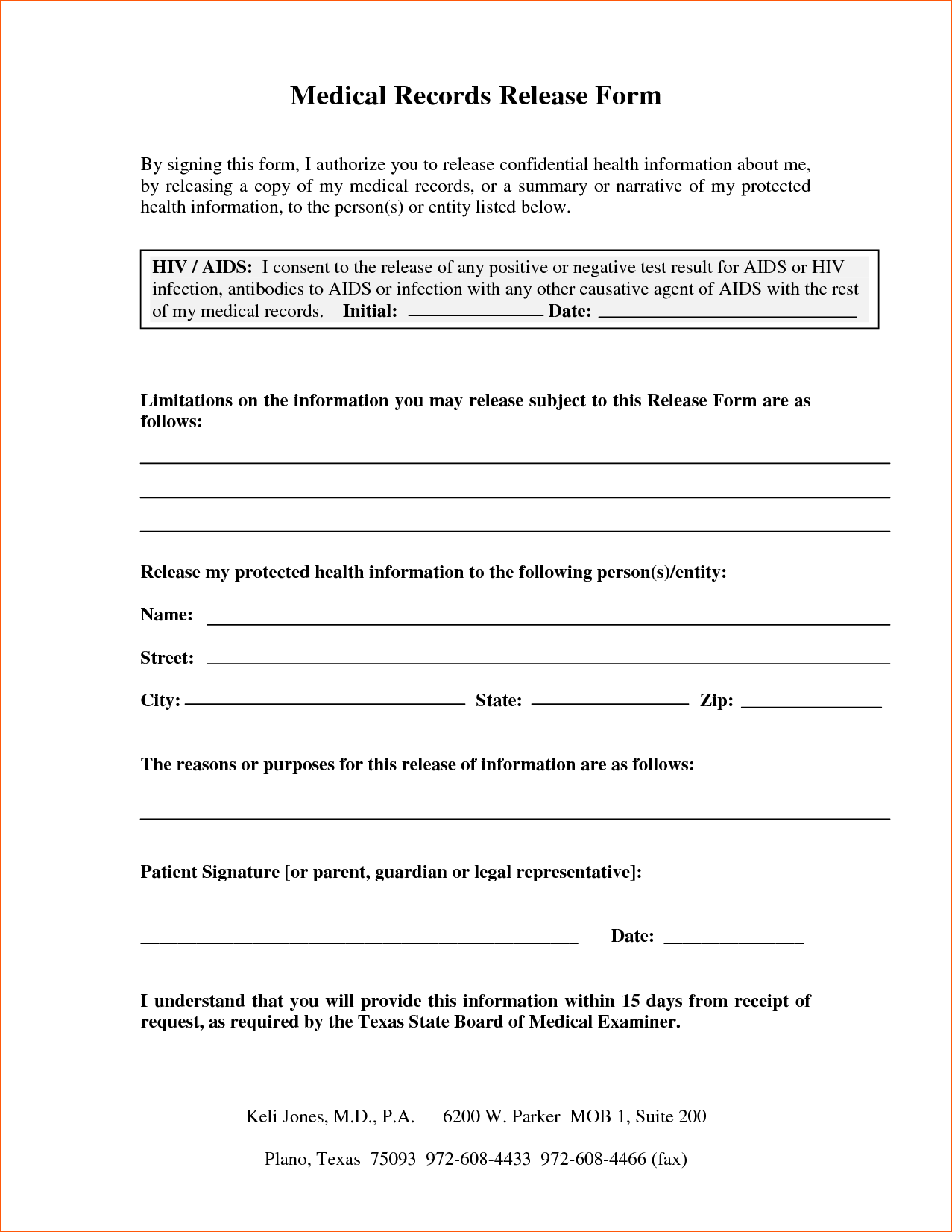
I authorize ________________________ (“authorized party”). This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. Write a medical records release authorization.
Printable Hipaa Forms For Patients Web Up To 40 Cash Back Printable
I authorize ________________________ (“authorized party”). To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. Write a medical records release authorization.
Medical Records Release Form templates free printable
I authorize ________________________ (“authorized party”). It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. A patient can also request their medical records not currently in their possession. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. It also allows.
Printable Medical Records Release Form
Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information. I authorize ________________________ (“authorized party”). This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards. A medical records release authorization form is a document that.
I Authorize ________________________ (“Authorized Party”).
A patient can also request their medical records not currently in their possession. It is essential to follow the state’s guidelines on how to craft the form to ensure that all essential. To request release of medical information please complete and sign this form i, ____________________________________hereby voluntarily authorize the disclosure of information from my health record. This form is for use when such authorization is required and complies with the health insurance portability and accountability act of 1996 (hipaa) privacy standards.
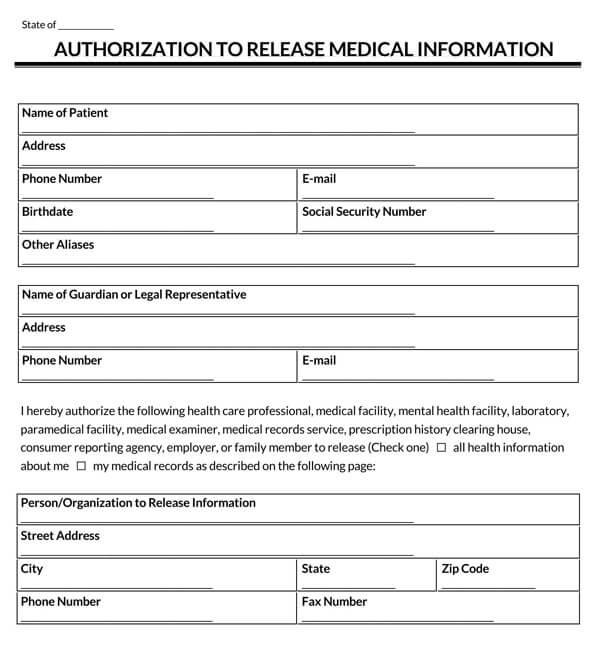
The Medical Record Information Release (Hipaa) Form Allows Patients To Give Authorization To A 3Rd Party And Access Their Health Records.
A medical records release authorization form is a document that allows a person to disclose protected health information to a third party. It also allows the added option for healthcare providers to share information. Write a medical records release authorization letter to the relevant office requesting the release, access, or transfer of health information.