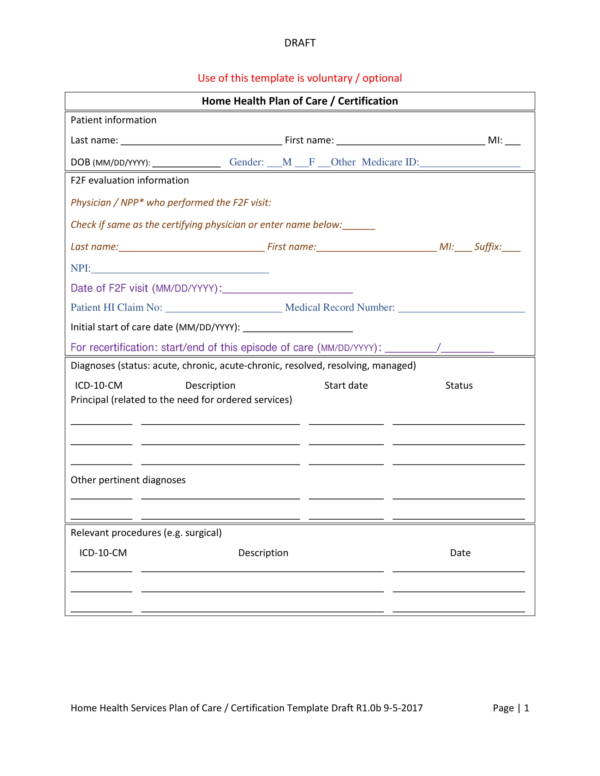
Home Health Order Template - This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Please explain the reason(s) the patient is confined to home: Home health orders initial certification and orders must be signed and dated by the ordering provider. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. Home health order form 7703 n. (md, pa, np) patient name:
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. Please explain the reason(s) the patient is confined to home: Home health orders initial certification and orders must be signed and dated by the ordering provider. Home health order form 7703 n. (md, pa, np) patient name:
Home health order form 7703 n. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health orders initial certification and orders must be signed and dated by the ordering provider. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. (md, pa, np) patient name: Please explain the reason(s) the patient is confined to home:
Home Health Order Template
Medical orders, recent falls, wheel chair bound, shortness of breath requiring. Home health order form 7703 n. (md, pa, np) patient name: This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health orders initial certification and orders must be signed and dated by the ordering.

How to Pay for Home Health Care
Home health order form 7703 n. Please explain the reason(s) the patient is confined to home: (md, pa, np) patient name: Home health orders initial certification and orders must be signed and dated by the ordering provider. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.

Home Health Plan Of Care Form 485
Home health orders initial certification and orders must be signed and dated by the ordering provider. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. (md, pa, np) patient name: Please explain the reason(s) the patient is confined to home: Medical orders, recent falls, wheel chair.
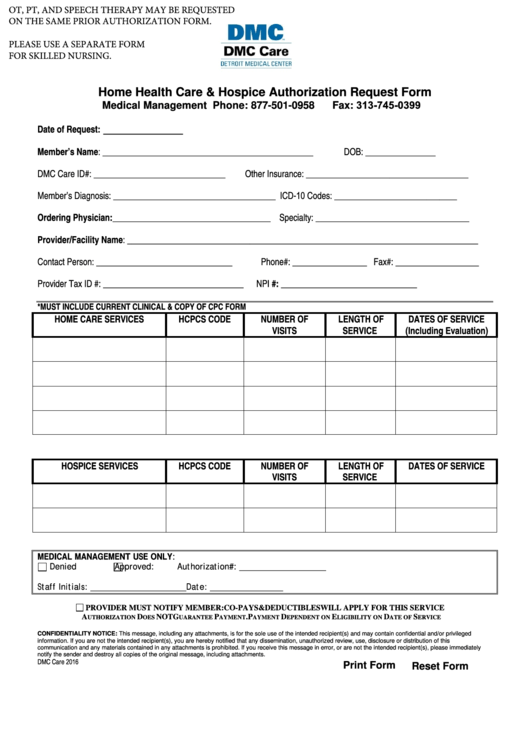
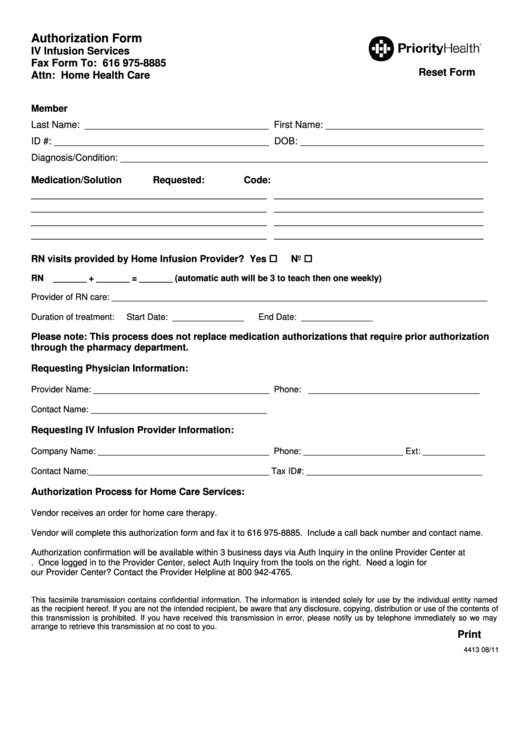
Fillable Home Health Care & Hospice Authorization Request Form
(md, pa, np) patient name: This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health order form 7703 n. Please explain the reason(s) the patient is confined to home: Home health orders initial certification and orders must be signed and dated by the ordering provider.

Home health physician order form Fill out & sign online DocHub
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health orders initial certification and orders must be signed and dated by the ordering provider. (md, pa, np) patient name: Home health order form 7703 n. Please explain the reason(s) the patient is confined to home:

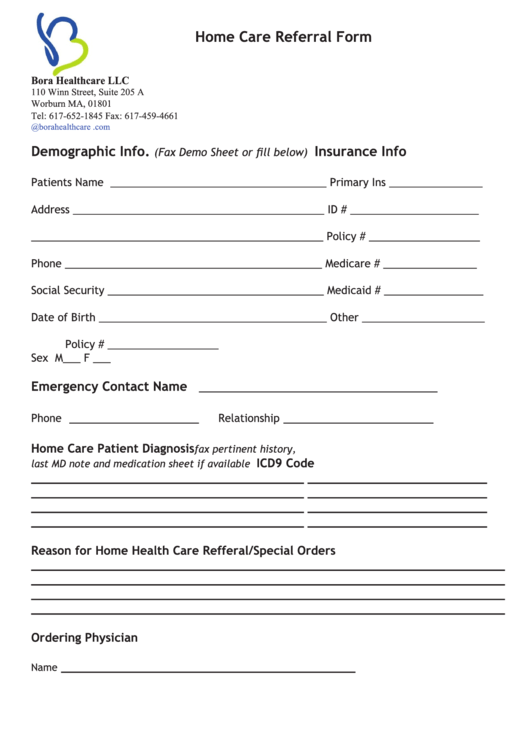
Printable Home Health Care Forms Templates
Home health order form 7703 n. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. (md, pa, np) patient name: Please explain the reason(s) the patient is confined to home:
21 Home Health Care Forms And Templates free to download in PDF
Medical orders, recent falls, wheel chair bound, shortness of breath requiring. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health order form 7703 n. Home health orders initial certification and orders must be signed and dated by the ordering provider. (md, pa, np) patient.
Home Health Order Template
Home health orders initial certification and orders must be signed and dated by the ordering provider. Home health order form 7703 n. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. (md, pa, np) patient name: Please explain the reason(s) the patient is confined to home:
Home Health Nurse Home Health Visit Form Template OASIS Etsy
This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the. Home health order form 7703 n. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. Please explain the reason(s) the patient is confined to home: Home health orders initial certification and orders must be signed.
Home Health Order Template
Please explain the reason(s) the patient is confined to home: Home health orders initial certification and orders must be signed and dated by the ordering provider. (md, pa, np) patient name: Home health order form 7703 n. This template has been designed to assist the physician in documenting the home health services plan of care / certification in establishing the.
Home Health Orders Initial Certification And Orders Must Be Signed And Dated By The Ordering Provider.
Home health order form 7703 n. Medical orders, recent falls, wheel chair bound, shortness of breath requiring. (md, pa, np) patient name: Please explain the reason(s) the patient is confined to home: